Changes in activity, speech, sleep, or the way a person moves are all examples of measurements that can be captured remotely using digital tools. If transformed into digital biomarkers, such remote measures could dramatically improve diagnosis and the testing of potential treatments in FTD. At the inaugural Holloway Summit in Miami, leaders in FTD research, industry, foundations, and technology discussed how to transform the tools already available into standardized digital biomarkers.
Digital Biomarkers of FTD: How to Move from Tech Tinkering to Trials?
Part 1 of 2
Kristin Holloway opened the inaugural Holloway Summit, held May 18-20 in Miami, by recounting her family’s experience with frontotemporal dementia (FTD). The events leading up to the diagnosis of her husband, Lee, may seem all too familiar to families grappling with the disease. As Kristin realized in hindsight, her husband’s behavior had started shifting long before, indeed, soon after their marriage and before the birth of their child. An ambitious tech entrepreneur who had co-founded the internet security company Cloudflare, Lee started sleeping in, skipping work, and lost interest in seeing friends. Like many spouses of people with FTD, Kristin initially chalked up her husband’s behavior to various stressors in his life. It took a visit from Kristin’s mother to make it painfully clear that something was wrong. After months of agonizing attempts to drag her reluctant husband to psychiatrists, and ultimately to neurologists, the family received the devastating diagnosis: Lee Holloway, at the age of 36, was suffering from behavioral variant FTD.
Kristin decided to do more about FTD than take care of her husband. She set up a fund with the Association for Frontotemporal Degeneration (AFTD). Part of her gift goes to funding an annual meeting around a specific goal, and for the initial one, that goal was accelerating the development of digital assessment tools for this disease.
Organized by AFTD, the summit brought together researchers in academia and industry, as well as business and nonprofit foundation leaders. The two days of talks and discussion brought experienced FTD investigators who are steeped in the confounding complexities of these diseases face-to-face with young entrepreneurs who have no patience for the slow pace of progress in this field.
While the first symptoms in FTD vary from person to person, one constant is that they only become clear to loved ones in hindsight, at a time when the affected person is far down the path of disease. Merely obtaining a diagnosis can be a challenge in this highly variable constellation of disorders. No disease-specific treatments exist. Clinical trials struggle to enroll sufficient numbers of participants, and to develop meaningful endpoints that capture the diverse manifestations of the disease. All this is why digital health technologies—which could reach anyone with a smartphone and keep tabs on the fluctuating symptoms of FTD—are so sorely needed. Having such markers would speed the path to treatments for the disorder.
Relative to its big cousin, Alzheimer’s disease, FTD is relatively rare, occurring in approximately 11 in 100,000 people. It is also marked by staggering heterogeneity at every turn, from its genetic causes to the type of pathology that spreads in the brain to the behavior, speech, and motor disturbances that arise. Behavioral variant FTD is the most common form, and some 40 percent of it is caused by an underlying pathogenic mutation. Primary progressive aphasias, which are most often sporadic, come in two forms marked by halting speech, or problems finding words or recognizing common objects. Certain movement disorders, including the atypical parkinsonian disorders corticobasal degeneration and progressive supranuclear palsy, and amyotrophic lateral sclerosis, also lie along the spectrum of frontotemporal lobar degeneration (FTLD), the pathological descriptor for this constellation of disorders.
Confusingly, many people develop symptoms of more than one type of clinical variant—for example, some people develop both bvFTD and ALS, while others suffer from a blend of behavioral and language symptoms. Vanishingly few specialists exist who can diagnose the disorder, let alone direct participants to clinical studies or trials. For the few who have found their way to a diagnosis, participation in clinical studies can become prohibitively burdensome as symptoms worsen, especially for those who live far from major medical centers.
And herein lies the potential of digital health technologies, said AFTD’s Penny Dacks. By developing digital tools to monitor symptoms from a participant’s home, scientists aim to dramatically expand access to clinical studies. Candidate digital biomarkers and other digital measures are currently being tested in international cohorts of pathogenic mutation carriers, and researchers hope that these will help pave the way to earlier detection and diagnosis among people with sporadic forms of the disease. Though improved diagnosis was not the main focus of this meeting, Dacks believes that objective digital measures that detect the subtlest of early symptoms may prove useful on that front.
Trouble is, although a plethora of researchers in academia and industry are at work to develop these tools, none have moved beyond the exploratory stage. “Folks working on innovation in technology have not always connected with folks working in the regulatory space,” Dacks said. “We need to have more cross-stakeholder discussion so we can move these tools beyond the idea stage.”
Rhoda Au of Boston University set the tone of the summit by calling for fundamental change in clinical research. For one, Au noted, the infrastructure needed to conduct clinical studies in the traditional way—in which patients visit a clinic and undergo a series of in-person evaluations with specialists—doesn’t exist in much of the world. China, for example, has roughly 300 neurologists for a population of 1.3 billion people, Au said. Large swaths of the world are excluded from clinical research.
As opposed to the scarce neurologist—let alone the elusive FTD specialist—the smartphone is ubiquitous even in developing countries. Within the next two years, 7 billion people are projected to hold these computers in the palms of their hands, Au said, making the smartphone the most penetrating technology in the world. With a further push from the COVID-19 pandemic, the use of smartphones and tablets has grown substantially even among the oldest ranks of the population. Capable of tracking myriad health and lifestyle factors that fluctuate from day to day, such devices have the capability to pick out emerging patterns from the chaos of daily life.
Some researchers translate traditional in-clinic tests, such as the neuropsychological inventory, into a digital format. Au takes a broader view of what should be done. Equipped with multiple sensors that would passively and continuously monitor a person’s daily habits, from movements within and outside of the house to sleep patterns to time spent with friends, smartphones can discern subtle changes in behavior that would go undetected by quarterly or biannual rounds of traditional in-clinic tests.
Frequent monitoring is well-suited to capturing changes associated with FTD, Au believes. At the earliest stages of neurodegenerative disease, symptoms crop up inconsistently, and different family members might report different sets of behaviors and symptoms. “That’s what digital biomarkers are going to have to mimic,” Au said. “This dynamic, changing set of signals comes together and reflects that there’s a real change happening.”
Bonnie Wong, a neuropsychologist at Massachusetts General Hospital in Boston, agrees that highly structured, traditional neuropsychological testing tends to miss the early symptoms of FTD. Wong said such tests are not “ecologically valid,” meaning they fail to capture what goes on in day-to-day life. Digital technology may unveil the fuller picture, one that matches what patients and their families are actually experiencing.
For example, bvFTD symptoms such as apathy, compulsion, and agitation could be detected simply by monitoring activity patterns. While an apathetic person may become planted on the couch, a compulsive or agitated person may pace back and forth right in front of it.
Rigging a willing person’s home with sensors that record their movements and behaviors is one way to capture signs that something is amiss. At the summit, Zach Beattie of Oregon Health Sciences University, Portland, described the ORCATECH (Oregon Center for Aging and Technology) monitoring platform. Funded by the Collaborative Aging Research Technology (CART) initiative, ORCATECH involves the placement of multiple in-home sensors and wearable devices that together track everything from a person's movement patterns within and outside the home, walking speed, sleep, computer and medication use, social time, and more. This surveillance is coupled with weekly online questionnaires that keep tabs on events that may have influenced changes in the readings—such as visitors in the home, falls, or hospital visits.
So far, the platform has been focused on changes in the run-up to Alzheimer's disease. For example, a recent study found that computer usage dropped off dramatically over two years in people with MCI, while healthy controls kept up their use. However, the platform is agnostic to which sensors are used, and new ones can easily be added to meet different goals, Beattie said.
Say Yes to Surveillance? The ORCATECH platform integrates data from multiple sensors, including wearable devices as well as sensors placed strategically around a person’s home. [Courtesy of Zach Beattie, OHSU.]
Research centers in the United States, as well as in Europe, Australia, India, and Taiwan, are deploying ORCATECH in their cohorts. Beattie said efforts are underway to transfer its massive amounts of data onto the cloud, where it can be accessed by researchers around the world.
Beattie thinks this multi-sensor approach is well-suited to pick up symptoms of FTD. With Jeffrey Kaye at OHSU, Beattie is collaborating with scientists at the University of California, San Francisco, on a pilot study to try out ORCATECH in the ALLFTD cohort, a multicenter observational study of familial and sporadic FTD ongoing in the United States and Canada (Mar 2021 news).
As presented by UCSF’s Adam Staffaroni at the Holloway summit, the pilot study will deploy ORCATECH across the spectrum of FTD, in 10 people with bvFTD, five with PPA, and five with PSP/CBS, along with 20 study partner controls. Participants will be monitored continuously for a year. The researchers hope to pick up changes in motor function, cognition, sleep, speech, and language over that time, pegging digital markers that track with disease progression and overall function.
Besides passive monitoring, ALLFTD is also implementing an FTD-tailored mobile app developed by Datacubed Health, which hosts a traditional battery of neuropsychological tests in digital form. The app is currently used in more than 45 clinical trials spanning different disorders, Staffaroni said. It runs on Android and Apple phones, and researchers can customize it with questionnaires and tasks that pertain to the goals of a given study. For the purposes of ALLFTD, the app currently includes tests of executive function, spatial memory, speech and language, and motor function, with tests of naming and semantic judgment in the works. To entice participants to complete these tasks, each is gamified with avatars, “virtual gems,” and links to Amazon gift cards.
After a pilot study deemed the app easy to use, ALLFTD initiated a Phase 2 trial; it has enrolled 223 participants across 18 centers so far. At the summit, Staffaroni presented preliminary results on 207 participants, comprising people with different variants of FTD in a range of stages. The scientists found that scores on the digital tasks correlated with scores of disease severity as gauged by the in-clinic CDR+NACC FTLD. This version of the clinical dementia rating scale has been adapted to include questions relevant to FTLD (Mar 2021 conference news).
Staffaroni's finding held true not only for new digital measures of executive function and spatial memory, but also for motor function. The scientists validated a remote version of the finger-tapping test—in which participants tap their phones as many times as possible in a short time window—as well as remote measures of gait and balance. These tests agreed with their in-clinic versions, and they correlated with disease severity.
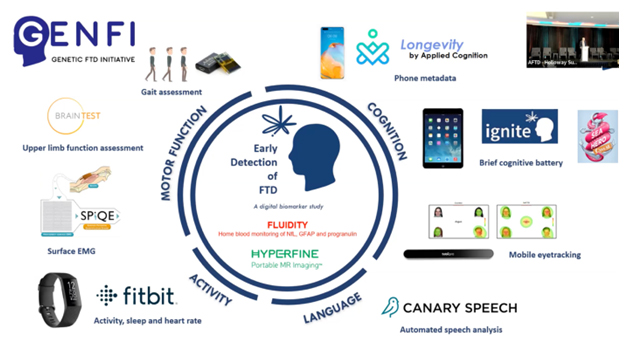
Jonathan Rohrer of University College London presented the current status of digital health technology development within the Genetic FTD Initiative (GENFI), a European-Canadian natural-history study of familial FTD. GENFI has done extensive work tracking behavioral, language, neuroimaging, and fluid biomarkers in its cohort, which includes both asymptomatic and symptomatic mutation carriers. Now, myriad tests are being deployed in digital form (see below).
Digital Palette. GENFI is validating digital tools that monitor cognition, language, activity, and motor function. [Courtesy of Jonathan Rohrer, UCL.]
In addition to passive monitoring, accelerometers, and other devices that track movements and physiology, GENFI has developed a tablet-based app that takes stock of cognitive function. Called Ignite, it includes gamified tasks that measure executive function, social cognition, and semantic memory. The entire battery takes 20-25 minutes to complete, with each task lasting no longer than 90 seconds, Rohrer said. So far, Ignite has been tested in 2,000 healthy controls, who showed slippage on some of the tasks with increasing age.
After verifying test-retest reliability of the app, Rohrer said Ignite will be rolled out to people with FTD, initially within the United Kingdom and then later in the wider GENFI cohort. Besides Ignite, tasks of social cognition and speech that have been developed by GENFI researchers in the clinic are being translated into mobile form, Rohrer said. This includes an eye-tracking test that follows a person’s gaze to assess how well they can recognize emotions in the faces of others.
One major domain of FTD symptoms that is noticeably absent from ALLFTD’s Mobile App or GENFI’s Ignite is behavior. Behavioral changes are difficult to capture in a test. They tend to come up in subjective reports from family members, and often go unnoticed by the person with FTD. At the summit, Michael Gold of AbbVie and other industry scientists urged the field to focus on developing more tools to assess behavioral change early on. Passive monitoring is one way to document these changes.
Speech is another domain that is amenable to digital monitoring and analysis. Naomi Nevler of the University of Pennsylvania, Philadelphia, reported that natural speech patterns may serve as clinical biomarkers that can tell apart types of FTD. Speech is the product of multiple neural networks working together, including networks that facilitate language, social cognition, executive, and motor function. Digitally recording acoustic, lexical, and rhythmic features of a person’s speech as they freely describe a picture—the classic example being the “cookie theft scene” (see below)—can bring to the fore deficits in these neural networks, Nevler said.
Notice Anything Strange? How a person describes the classic “cookie theft” scene can signal the presence of FTD to a clinician. Now, digital tools that monitor different features of speech may distinguish between different variants of FTD. [Courtesy of Naomi Nevler, UPenn.]
For example, people with semantic variant PPA, who have difficulty naming objects, relied on pronouns or ambiguous nouns to describe objects in the picture that they were unable to name. People with non-fluent, agrammatic PPA paused often, and tended to utter more partial words (Cho et al., 2021). Even people with behavioral variant FTD—who do not suffer from a language disorder, per se—had a speech signature, in that they spoke within a narrow acoustic range. This fits with the observation that people with bvFTD tend to speak in a monotone voice. People with this variant also spoke in shorter segments, with longer pauses than healthy controls, in keeping with their symptoms of apathy and distraction. Nevler was able to tie all these different speech signatures to atrophy in corresponding regions of the brain.
The findings suggest that speech harbors a wealth of information about dysfunction in different regions of the brain and can even differentiate among clinical variants of FTD. Nevler said these speech measurements are currently being deployed via tablets and smartphones in the clinic and remotely via a virtual conference app. The recording sessions last but a few minutes. What’s more, automated speech-analysis methods are more objective and quantifiable than a human listener, suggesting they might work as biomarkers in clinical trials. “I see different digital-speech features supporting all elements of patient care,” Nevler told Alzforum. “This includes screening, diagnosis, monitoring, prognosis (risk assessment), and support for patient quality of life at home.”
Commercial speech-assessment tools have started making their way into clinical trials as exploratory measures. Jessica Robin of Winterlight, a Toronto-based company that develops tablet-based speech-assessment tools, reported that people with FTD have distinct speech patterns that correlate with clinical decline. The tablet-based Winterlight speech composite, which is in use as an exploratory endpoint in AD clinical trials, scores some 500 vocal features, including acoustics, speed, types of words used, vocabulary, fluency, and sentence construction. Robin previously reported that over one year of regular assessments, the app picked up changes in speech in people with FTD, including those with the behavioral variant (Dec 2021 news). Winterlight’s speech-assessment tool is being used as an optional, exploratory measure in Alector’s INFRONT-3 trial, which is evaluating the progranulin-boosting monoclonal antibody AL001 in people with FTD who carry a pathogenic mutation in the gene.
With so many digital gadgets and measures to choose from, how can the FTD field come together to push the best ones forward? In Part 2 of this series, read about how scientists in related neurodegenerative disease fields have fared, and the major challenges that stand in the way of worldwide implementation of digital biomarkers.—Jessica Shugart
Digital Tools Abound, Yet Remote Biomarkers for FTD Remain Exploratory
Part 2 of 2
Frontotemporal dementia is a wildly heterogeneous group of disorders, and many people with an FTD have difficulty getting an accurate diagnosis, let alone proper care or treatment. Digital biomarkers would expand access to services and speed therapy development. In recent years, sophisticated tools have been created that can track everything from movement to sleep patterns, social life, speech features, memory, balance, and beyond. At the inaugural Holloway Summit, held May 18-20 in Miami, leaders across the field of FTD and related disorders came together to discuss what has been developed so far, and how to streamline the technological offerings into standardized, validated digital biomarkers that reliably aid in diagnosis, prognosis, and clinical trials (see Part 1 of this series).
Fit for Purpose
At this point, most digital FTD markers are in the research or validation phase, and are not yet in use in clinical trials. That said, a broad array of digital measures, devices, and apps are being tested by different groups across the world. “How do we best leverage all of these digital technologies to accelerate treatment development?” Adam Boxer of the University of California, San Francisco, asked the audience. He thinks it’s crucial to sort out which markers best fit defined, given purposes, such as diagnosis, prognosis, or tracking treatment effects. It will also be critical to harmonize digital health technologies across observational cohorts.
Together with Jonathan Rohrer at University College, London, Boxer heads the FTD Prevention Initiative, a global collaboration between FTD cohorts. It includes ALLFTD, GENFI, Australia’s Dominantly Inherited Non-Alzheimer Dementias (DINAD) study, New Zealand’s FTD Genetic (FTDGeNZ) study, and South America’s Research Dementia Latin America (ReDLaT) study (Mar 2021 news). Selecting digital markers that can be deployed across cultures will be essential for conducting global research studies and clinical trials in this initiative, particularly in countries where most people lack access to medical centers, Boxer emphasized.
Is there any sign yet of harmonization between the flurry of devices and measures that are in the works? ALLFTD and GENFI are planning a pilot study in which they swap apps, trying out the ALLFTD Mobile app in the GENFI cohort and the Ignite app in the ALLFTD cohort (see Part 1). Boxer wants to do this on a larger international scale in FPI, he told Alzforum, but acknowledged that it took ALLFTD and GENFI years just to integrate their basic data on age at symptom onset and disease duration (Moore et al., 2020). “We have to anticipate this with digital measures,” Boxer said. He emphasized that data needs to be shared broadly to accelerate the advance of digital markers, and yet, agreeing on ways to share complex and sensitive data continues pose significant challenges for the field.
Path to Patients: Learning from Parkinson's
In its quest to streamline digital technologies and measures into a few broadly usable tools, the FTD field can learn from the trials and tribulations in Parkinson's disease, ALS, and Alzheimer's disease. The Holloway Summit featured talks about digital technology development in these disorders, all of which have some overlap with FTD.
Diane Stephenson, who founded the Critical Path for Parkinson’s (CPP) Consortium, told the audience that data sharing on a global scale, involvement of regulatory agencies at every step along the way, and listening seriously to patients are essential if digital health technology development is to succeed. Founded seven years ago, CPP convenes leaders in academia, industry, foundations, regulatory agencies, governmental organizations, and people with PD. CPP has integrated data from more than 15,000 participants in PD research studies and clinical trials. With this data, the consortium is designing PD clinical trials, and looking for biomarkers that can enrich trials with people in the earliest stages of disease. Digital health technologies are chief among the consortium’s goals, Stephenson said.
PD has been the flagship disease for digital tools because, to tech people, tracking movement symptoms with built-in accelerometers seems like a no-brainer. “But PD is not that simple,” Stephenson said. Even in its earliest stages, patients have non-motor symptoms, including restless sleep, pain, fatigue, and changes in mood and cognition, which are rarely included as primary endpoints in clinical trials. To develop digital tools for early PD, CPP formed the industry, academia, and patient advocacy consortium 3DT. It uses an open, precompetitive model to transform digital tools from siloed, exploratory measures into standardized biomarkers that can be put to broad use in clinical trials (Stephenson et al., 2020; Stephenson et al., 2021).
Take, for example, the Wearable Assessments in the Clinic and Home in PD (WATCH-PD) study. With Biogen and Takeda, along with University of Rochester scientists Ray Dorsey, Jamie Adams and Jennifer Mammen, 3DT compared in-clinic assessments to those taken remotely via a combination of smartwatch and smartphone. Using these wearable devices equipped with motion sensors, microphones for recording speech, as well as participant questionnaires, researchers monitored a range of motor and non-motor symptoms from afar.
Initially, the study was going to include people with early PD who showed signs of dopamine deficiency via DaT scan. However, after consulting with the FDA prior to the start of the study, the investigators added a control group. They also took a hint from a public rejection letter the FDA had posted in response to an application by Verily. That company had developed a digitized version of the MDS-UPDRS Part III, considered the gold standard measure of motor symptoms. The regulators wrote that the digitized MDS-UPDRS Part III “cannot be interpreted as being meaningful to patients.” To avoid the same fate, the WATCH-PD investigators worked with the FDA to devise an extensive exit interview for participants that would help them discern which digital measurements most closely link to aspects that are important in their lives. Stephenson said those interviews are ongoing.
Preliminary findings from the WATCH-PD study are promising, Stephenson reported. For example, by picking up a reduced arm swing, the smartwatch could tell the difference between people with PD and controls. This is a big deal, Stephenson said, because these participants were at such an early stage. It also corroborates previous studies in pathogenic LRRK2 mutation carriers, whose arm swing changed while they were presymptomatic (Mirelman et al., 2016).
Stephenson said that the WATCH-PD study is an example of how this kind of collaboration can work. Such large collaborative efforts are needed to advance digital health technologies in FTD, as well, she believes.
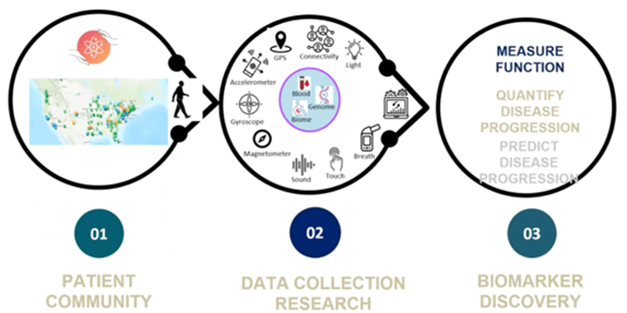
One new example of an open-science, all-hands-on-deck approach is Everything ALS. Founded in 2020 by Indu Navar, a tech entrepreneur whose husband died from the disease in 2019, EALS is a nonprofit organization featuring a global online platform through which people with ALS can engage in studies. By bringing together patients from around the world, ALS researchers in academia and industry, and tech and device companies, EALS aims to develop digital biomarkers that will support early diagnosis of ALS and make clinical trials more efficient. At the Holloway summit, Navar emphasized that even for people like her husband, who had access to the best medical care, merely obtaining an ALS diagnosis was a long process. After that, the measures used to track his disease progression were subjective and lacking in sensitivity.
Navar formed an international patient network that runs studies on digital tools. Its nearly 5,000 participants take part in studies to try out different digital measures. The measurements and technologies EALS explores include structured and natural speech analysis, video tracking of facial movements, monitored internet search behavior, and measuring subtle differences in the way people use their keyboard mouse.
With the help of artificial intelligence, EALS is amassing a dataset meant to be open to researchers in academia and industry. For example, the EALS speech and facial study, which is hunting for ALS-specific signals in speech and facial gestures, includes 750 participants so far. They have taken part in 6,000 sessions yielding 1,000 hours of data, which is analyzed in partnership with artificial intelligence companies and shared with pharma and academic researchers, Navar reported.
All studies run through the platform are IRB-approved, and participants consent to having their data be shared in de-identified form. They can access their own data, because this type of transparency is essential for keeping people engaged in the study, Navar said.
Path to Biomarkers? Using an online platform and partnering with Microsoft, IBM, modality.ai, pharma companies, and medical centers, EALS boasts a growing community of people with ALS, who are joining studies of potential digital health technologies for diagnosis, prognosis, and clinical trials. [Courtesy of Indu Navar, EALS.]
BYOD or Take the Study's?
Digital biomarker developers wrestle with the question of whether to design tests to work on a participant’s device—“bring your own device” (BYOD)—or to give participants a specialized study device. The advantage of BYOD is self-evident—most people have a smartphone these days, and who wants to carry another? However, developing digital tools that work consistently across different types of smartphone is not trivial, as Jason Hassenstab of Washington University in St. Louis can attest.
At the summit, Hassenstab described his team's challenges in developing a smartphone app for global trials for the growing Dominantly Inherited Alzheimer's Network Trials Unit (DIAN-TU). Called the Ambulatory Research in Cognition (ARC) app, it enables daily testing of a user’s spatial memory, processing speed, and associative memory in less than three minutes per session (Aug 2018 conference news). Besides ensuring that the tasks work across languages and cultures, Hassenstab grappled with differences in smartphones, of which more than 19,000 models exist worldwide. For one, tap latency—the time it takes for a phone to register a finger tap—varies markedly between phones, especially those with different operating systems. Even among phones with the same operating system, tap latency can change after a routine software upgrade, or if the phone is in power-saving mode, Hassenstab reported. This spurred Hassenstab to shift away from tasks that rely on response time, and focus on correct answers instead (Aug 2019 news).
Researchers also need to consider how smartphone access varies by demographics. Many people who live in rural areas, or those with low socioeconomic status, lack access to a Wi-Fi signal, and Androids are more common globally than pricier Apple iOS phones.
Despite the challenges, the summit's attendees agreed that digital biomarkers and, ultimately, digital endpoints for clinical trials will be necessary to find effective treatments for FTD. To Boxer, such tools are the key to running global clinical trials. His dream? An app that could be downloaded onto any smartphone, with a culturally harmonized, common set of endpoints. “The technology exists, and I’m naively optimistic that we can make it happen,” Boxer said.—Jessica Shugart
Moore KM, Nicholas J, Grossman M, McMillan CT, Irwin DJ, Massimo L, Van Deerlin VM, Warren JD, Fox NC, Rossor MN, Mead S, Bocchetta M, Boeve BF, Knopman DS, Graff-Radford NR, Forsberg LK, Rademakers R, Wszolek ZK, van Swieten JC, Jiskoot LC, Meeter LH, Dopper EG, Papma JM, Snowden JS, Saxon J, Jones M, Pickering-Brown S, Le Ber I, Camuzat A, Brice A, Caroppo P, Ghidoni R, Pievani M, Benussi L, Binetti G, Dickerson BC, Lucente D, Krivensky S, Graff C, Öijerstedt L, Fallström M, Thonberg H, Ghoshal N, Morris JC, Borroni B, Benussi A, Padovani A, Galimberti D, Scarpini E, Fumagalli GG, Mackenzie IR, Hsiung GR, Sengdy P, Boxer AL, Rosen H, Taylor JB, Synofzik M, Wilke C, Sulzer P, Hodges JR, Halliday G, Kwok J, Sanchez-Valle R, Lladó A, Borrego-Ecija S, Santana I, Almeida MR, Tábuas-Pereira M, Moreno F, Barandiaran M, Indakoetxea B, Levin J, Danek A, Rowe JB, Cope TE, Otto M, Anderl-Straub S, de Mendonça A, Maruta C, Masellis M, Black SE, Couratier P, Lautrette G, Huey ED, Sorbi S, Nacmias B, Laforce R Jr, Tremblay ML, Vandenberghe R, Damme PV, Rogalski EJ, Weintraub S, Gerhard A, Onyike CU, Ducharme S, Papageorgiou SG, Ng AS, Brodtmann A, Finger E, Guerreiro R, Bras J, Rohrer JD, FTD Prevention Initiative.
Age at symptom onset and death and disease duration in genetic frontotemporal dementia: an international retrospective cohort study.
Lancet Neurol. 2020 Feb;19(2):145-156. Epub 2019 Dec 3
PubMed.
Stephenson D, Alexander R, Aggarwal V, Badawy R, Bain L, Bhatnagar R, Bloem BR, Boroojerdi B, Burton J, Cedarbaum JM, Cosman J, Dexter DT, Dockendorf M, Dorsey ER, Dowling AV, Evers LJ, Fisher K, Frasier M, Garcia-Gancedo L, Goldsack JC, Hill D, Hitchcock J, Hu MT, Lawton MP, Lee SJ, Lindemann M, Marek K, Mehrotra N, Meinders MJ, Minchik M, Oliva L, Romero K, Roussos G, Rubens R, Sadar S, Scheeren J, Sengoku E, Simuni T, Stebbins G, Taylor KI, Yang B, Zach N.
Precompetitive Consensus Building to Facilitate the Use of Digital Health Technologies to Support Parkinson Disease Drug Development through Regulatory Science.
Digit Biomark. 2020;4(Suppl 1):28-49. Epub 2020 Nov 26
PubMed.
Mirelman A, Bernad-Elazari H, Thaler A, Giladi-Yacobi E, Gurevich T, Gana-Weisz M, Saunders-Pullman R, Raymond D, Doan N, Bressman SB, Marder KS, Alcalay RN, Rao AK, Berg D, Brockmann K, Aasly J, Waro BJ, Tolosa E, Vilas D, Pont-Sunyer C, Orr-Urtreger A, Hausdorff JM, Giladi N.
Arm swing as a potential new prodromal marker of Parkinson's disease.
Mov Disord. 2016 Oct;31(10):1527-1534.
PubMed.



Comments
No Available Comments
Make a Comment
To make a comment you must login or register.