Dare We Say Consensus Achieved: Lecanemab Slows the Disease
Quick Links
The top-line results last September from Eisai’s Phase 3 trial of the anti-amyloid antibody lecanemab galvanized the field, but scientists said they needed to see the data before passing judgement. Now they have. At the 15th Clinical Trials on Alzheimer’s Disease conference, held November 29 to December 2 in San Francisco and online, scientists presented detailed findings to a standing-room-only audience of some 2,000 people and many more on livestream. Four speakers reported that secondary and biomarker measures were consistent, and of similar magnitude to the effect on primary. Overall, lecanemab appeared to slow disease progression by about one-quarter, and caused the brain edema known as ARIA-E in one of eight participants. The data were published in the New England Journal of Medicine November 29, the same day as the presentation.
- On lecanemab, all clinical outcomes showed similar slowing of decline.
- Amyloid plaque dropped below 25 centiloids after 18 months.
- AD biomarkers fell; neurodegeneration markers were mixed.
The audience responded positively. Many scientists praised the trial’s execution, and expressed relief that the presentations appeared thorough and transparent. “The Clarity trial is a landmark in AD therapeutic research, the culmination of over three decades of efforts across the field,” said Paul Aisen of the University of Southern California in San Diego. Randall Bateman of Washington University, St. Louis, presented the biomarker evidence, concluding that it indicates the treatment modified underlying biology. “These findings support the ability to change the course of Alzheimer’s disease,” he told Alzforum. Takeshi Iwatsubo of the University of Tokyo agreed, saying “This is a monumental event for patients.” All three are co-authors on the NEJM paper. Other researchers mentioned aspects of the trial design that strengthened their confidence in the findings, such as Eisai using separate medical teams to handle participants’ clinical trial evaluations and ARIA to minimize the risk of unblinding.
At the same time, researchers said the ARIA risks need to be taken seriously, and stressed that not all patients will be candidates for this therapy. Everyone agreed on the need to build on a small effect size by adding other therapeutic approaches and finding ways to give lecanemab earlier in disease.

Diverging Trajectories. People on lecanemab worsened more slowly on the CDR-SB than did people on placebo, resulting in a quarter less progression at 18 months. [Courtesy of Eisai.]
A Consistent Clinical Benefit
The 18-month Clarity trial enrolled 1,795 people with mild cognitive impairment or mild dementia due to AD, half of whom received 10 mg/kg intravenous lecanemab every two weeks. Eisai previously reported that lecanemab slowed decline on the primary outcome measure, the CDR-SB, by 0.45 points on the 18-point scale, or about one-quarter of the 1.66-point decline seen in the placebo group (Sep 2022 news).
In San Francisco, Christopher van Dyck of Yale School of Medicine in New Haven, Connecticut, fleshed out details on secondary measures. These mirrored the CDR-SB, with participants on lecanemab declining 1.44 fewer points on the ADAS-Cog14 and 0.05 fewer on the ADCOMS than the placebo group, for relative slowings of 26 and 24 percent, respectively. On a functional measure, the ADCS MCI activities of daily living (ADL), lecanemab put on the brakes by 2 points, or 37 percent. For all four clinical measures, the difference between lecanemab and placebo became statistically significant by six months and grew over time. On the CDR-SB and ADL, the slopes continued to diverge up to 18 months, whereas the difference between the curves appeared to stabilize on the ADAS-Cog14 at 15 months, and on the ADCOMS at 12.
“Because there is such mild decline in these patients over 18 months, it’s very difficult to see a positive signal,” noted Eric Musiek of Washington University in St. Louis, adding, “I’m impressed the signal is so clear, even if it is small in an absolute sense.”
The slightly larger effect on ADLs caught the interest of some scientists, since these can feel most important to participants. “[This] indicates that patients and families could benefit from slowing of observable functional worsening,” Joshua Grill of the University of California, Irvine, wrote to Alzforum (full comments below).
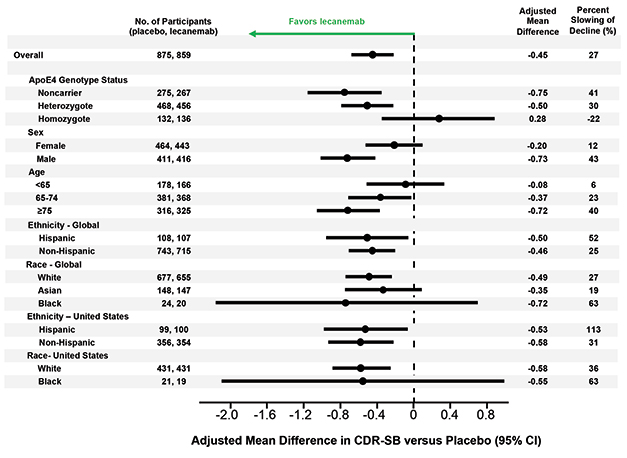
Left of Center. Lecanemab had similar effects in all subgroups examined, though men appeared to benefit more than women, older people more than younger, and APOE4 non-carriers more than carriers. [Courtesy of Eisai.]
Van Dyck also showed results from several sensitivity analyses that suggested the findings were not caused by confounding factors. In the treatment and placebo groups, 81 and 84 percent of participants, respectively, completed the trial, but dropouts did not affect the results. Imputing missing data and accounting for the COVID-19 pandemic did not change the data either. Nor did removing data from participants who developed ARIA-E, suggesting the positive results were not due to inadvertent unblinding of participants.
Likewise, subgroup analyses breaking down participants by age, sex, race, ethnicity, geographic region, disease stage, and use of symptomatic AD medications found treatment benefits across the board. Women appeared to benefit somewhat less than men, a potential difference that sparked discussion in the field. One possibility is that women have more advanced tau pathology at a given stage of cognitive impairment than men, making amyloid removal less effective for them, Maria Teresa Ferretti of the Women's Brain Project, a global non-profit based in Guntershausen, Switzerland, told Alzforum (Nov 2019 news).
The researchers also found a difference by APOE genotype. APOE4 carriers made up two-thirds of the cohort, and seemed to benefit less from lecanemab than noncarriers. In particular, the 15 percent of participants who carried two copies of APOE4 appeared to post no treatment effect on the CDR-SB, and but a small one on the ADAS-Cog14 and ADCS MCI-ADL. However, several scientists told Alzforum that they suspect the homozygote finding represents statistical noise. They pointed out that APOE4 homozygotes on placebo barely declined during the trial, muddying the ability to see a treatment effect in this small subgroup.
Colin Masters of the University of Melbourne, Australia, believes greater effects of lecanemab in APOE4 noncarriers make sense. “We know APOE4 leads to amyloid deposition starting earlier in life than in E4 noncarriers. I suspect the noncarriers had a better result because they started out with a lower amyloid burden,” Masters told Alzforum. He suggested letting trials run longer than 18 months to better detect effects in carriers.
The findings contrast with data from aducanumab, where more of the cognitive benefit in the positive EMERGE trial occurred in APOE4 carriers (see Nov 2020 news).
The Pesky Question: Does This Help Patients?
As with the FDA approval of aducanumab in June 2021, researchers at CTAD debated whether the measured benefit on these clinical tests is clinically meaningful. Sharon Cohen of the Toronto Memory Program, a site investigator for the Clarity trial, argued that it is. She noted that participants on lecanemab and their caregivers reported from one-quarter to one-half less worsening on measures of quality of life and caregiver burden compared to the placebo group. Looking at the data another way, the slower decline translated to a one-third lower risk of advancing to the next stage of AD during the trial, Cohen said.

More Time. Alzheimer’s disease progressed more slowly in people on lecanemab, delaying arrival of the next disease stage. [Courtesy of Eisai.]
This equates to a five- to six-month delay in disease progression, said Eric Siemers of Siemers Integration LLC (full comment below). Others noted this is similar to the benefit of acetylcholinesterase inhibitors, and wanted a Cohen’s d analysis of effect size for easier comparison with other treatments.
Researchers agree that the key question is what happens when people stay on lecanemab for longer periods. Will the clinical benefit persist, grow, as many argue, or diminish? Clinicians are eager to see data from open-label extension studies that might answer this question. “If the reduction in decline were to persist for, say, three to four years, I would expect it to be appreciated by families and patients. On the other hand, if the effect is not durable and fades within a year or so, there will be much less enthusiasm for its use, which after all is somewhat arduous,” David Knopman of the Mayo Clinic in Rochester, Minnesota, wrote to Alzforum (full comment below).
Amyloid as Surrogate?
As expected, lecanemab’s slashing of plaque was dramatic. In Clarity, participants started with an average amyloid PET of 76 centiloids at baseline. This rose by four in the placebo group and dropped by 55 in the treatment group, for a difference of 59 centiloids at 18 months. The divergence between groups became statistically significant at three months, and another three months later clinical measures started changing. Participants on lecanemab ended up with an average of 23 centiloids, which is below the threshold for amyloid positivity typically set at 25. Put another way, two-thirds of the treatment group became PET amyloid-negative at 18 months.
Roger Nitsch of Neurimmune, Switzerland, believes there is also a threshold effect for clinical benefit. In a keynote talk at CTAD, he noted that positive trials of anti-amyloid antibodies, such as Clarity, aducanumab’s EMERGE, and donanemab’s TRAILBLAZER, all brought plaque below 25 centiloids. Negative trials, such as aducanumab’s ENGAGE and the recent GRADUATE studies of gantenerumab, did not. “We have to lower amyloid load to 25 or less to get a clinical effect,” Nitsch proposed.
Others concurred that the relationship between amyloid removal and clinical benefit may not be linear, but stepwise. Eisai has not yet shown data on the correlation between how much of a person’s plaque vanished and their clinical response in Clarity. Ron Petersen of the Rochester Mayo Clinic said that more data are needed on whether it makes a difference how fast amyloid was removed.
At CTAD, researchers debated whether the Clarity results are strong enough to validate plaque removal as a surrogate biomarker for disease slowing. Maria Carrillo of the Alzheimer’s Association made a case for this; others want to see more data. Van Dyck noted that plaques could well be a stand-in for smaller aggregates, which might be the toxic species responsible for cognitive decline. Grill suggested that downstream markers of tangle burden and neurodegeneration may be more important for predicting the cognitive effects of treatment.
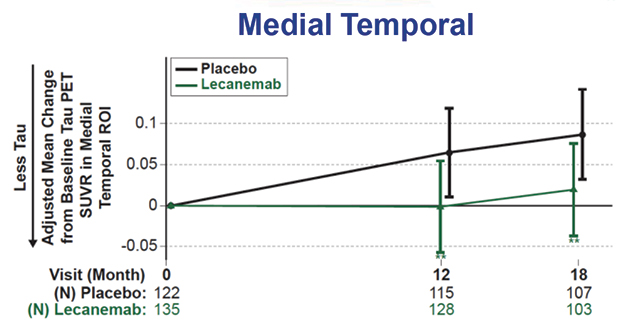

Tangle, Inflammation Markers Down. Tau tangle spread slowed on lecanemab (top), while a fluid marker of astrogliosis fell (bottom). [Courtesy of Eisai.]
Alzheimer’s Biomarkers Down, Neurodegeneration Signals Mixed
Regarding those markers, CTAD provided a wealth of data. Bateman reported that on lecanemab, the Aβ42/40 ratio rose by about 60 percent in cerebrospinal fluid and 10 percent in plasma, while p-tau181 dropped around 16-18 percent in both. These measures became statistically different from placebo at six months, in tandem with the clinical benefits. Tau PET showed a slowing but not stoppage of tangle accumulation in the medial temporal lobe, and trends toward slowing in other brain regions, with the PET signal increasing about half as much as in controls. The astrogliosis marker GFAP fell about 15 percent on lecanemab, but rose 10 percent in those on placebo.
“I was particularly pleased to see the significant fall in plasma GFAP levels,” Dennis Selkoe of Brigham and Women’s Hospital, Boston, wrote to Alzforum. “This suggests a notable amelioration of an inflammatory component that is increasingly recognized as a main feature of AD.”
Neurodegeneration markers gave a more ambiguous picture. CSF total tau fell about 4 percent on lecanemab, while rising 15 percent on placebo. Neurogranin, which reflects synapse loss, normalized as well, falling about 15 percent. On the other hand, plasma NfL only trended toward improvement on lecanemab, while CSF NfL did not change.
As has been seen with other amyloid immunotherapies, structural MRI revealed more shrinkage of whole brain and of cortical thickness on lecanemab, and an expansion of the brain's fluid-filled ventricles. Curiously, however, atrophy in the much smaller hippocampal region slowed. Brain atrophy used to be considered bad, and is used routinely as a diagnostic aid for many brain diseases. Alzheimerologists still do not know what to make of these findings. An early hypothesis—that gray matter shrinkage may reflect amyloid removal—is not in vogue anymore, but nothing else has emerged in its place. Knopman cautioned that the increase in ventricle size in particular deserves further study. “We are willing to ignore this finding now because we have a clinical benefit, which is the gold standard. But we need to keep it in mind,” he said.
Overall, the data support the idea that lecanemab modifies underlying biology, Bateman said. Eric Reiman of Banner Alzheimer’s Institute in Phoenix, whose abiding interest is in enabling prevention, believes these data will help facilitate future prevention trials for a range of drugs by clarifying how biomarker changes predict clinical outcomes.
ARIA Lower, but the Risk Is Real
Safety is a major concern for the widespread use of any amyloid immunotherapy. Eisai and Biogen previously announced that 12.6 percent of people taking lecanemab developed the brain edema known as ARIA-E. In San Francisco, Marwan Sabbagh of the Barrow Neurological Institute in Phoenix showed details. About one-quarter of ARIA-E cases came with symptoms, which were typically mild and cleared up within three to six months. Three people in the trial had severe symptoms, though Sabbagh did not identify what they were.
As expected, a person's ARIA-E risk was driven by his or her APOE genotype. One-third of APOE4 homozygotes developed ARIA-E, compared to 10 percent of heterozygotes and 5 percent of noncarriers. For reference, in aducanumab’s Phase 3 trials, those percentages were 66, 36, and 20 (Dec 2021 news).
Researchers said the overall risk/benefit calculation favors lecanemab. “I view the safety profile to be acceptable,” Grill said. Nick Fox of University College London agreed. “Any risk is clearly important, but I believe many of my patients would be willing to take such a risk,” he wrote (full comment below).
Nonetheless, they cautioned that clinicians will need to understand well what concurrent illnesses might magnify their patients’ risk so they can counsel them appropriately. Recent reports of two deaths from brain hemorrhage in the lecanemab open-label extension have broadly publicized the issue. One was a man with atrial fibrillation who was taking blood thinners; the other, a woman with cerebral amyloid angiopathy who received tissue plasminogen activator after a stroke (see Science story).
Neither death has been definitively linked to lecanemab, but they have reignited discussion about whether blood thinners and tPA should be contraindicated for people taking lecanemab. Anticoagulant use was allowed in the Clarity trial, in part because Eisai felt it needed to collect these data to learn about the issue, Eisai’s Mike Irizarry told the audience during his presentation. Macrohemorrhages, defined as any brain bleed larger than 1 cm, came in at 0.7 percent in the treatment group, higher than the 0.2 percent in the placebo group. For people on anticoagulants, the rate of macrohemorrhage on lecanemab was 2.4 percent, a more than threefold increase.
“tPA and anti-Aβ antibodies perhaps should not be given to the same AD patient, especially in the presence of CAA,” said Mathias Jucker, Hertie Institute, Tuebingen. Twenty years ago, Jucker’s group described how both tPA and Aβ immunotherapy induced cerebral bleeding in mouse models with CAA, though the scientists did not test the combination (Winkler et al., 2002; Pfeifer et al., 2002).
Stepping Stone to Disease Modification?
With a decision on accelerated approval of lecanemab scheduled by January 6, researchers expect the drug to become clinically available in 2023 (Jul 2022 news). Fox noted that this will create a tremendous challenge for healthcare systems, which at present lack the resources to do the diagnosis, counseling, imaging, IV infusions, and MRI monitoring needed. Most clinics are unprepared to roll out amyloid immunotherapy quickly at a large scale.
Even so, researchers at CTAD liked that the Clarity cohort was more representative of the general AD population than were previous trial cohorts. It included 22.5 percent Hispanic and 4.5 percent black participants. The age range was broad, from 50 to 90 years old, and inclusion criteria were intentionally liberal, allowing people with common conditions such as hypertension, diabetes, obesity, hyperlipidemia, and heart disease to join. Selkoe noted that about one-fourth of AD patients in the general population would meet the Clarity inclusion criteria, suggesting many could qualify for lecanemab treatment.
Still, clinicians are cautious. “If I were to start using this in my clinic, I would target it at healthier patients with positive biomarkers but milder symptoms, less atrophy on MRI, no microhemorrhages, and no anticoagulation,” Musiek wrote. “Patients will need to be motivated, reliable, and have good access and support (as well as insurance) to successfully receive this therapy and keep up with the MRI monitoring.”
The Alzheimer’s Association in 2021 announced a registry study, dubbed ALZ-NET, to track the long-term risks and benefits of disease-modifying AD therapies (Nov 2021 conference news; Aug 2022 conference news). In San Francisco, Carrillo noted that ALZ-NET enrolled its first patient November 1. So far, all participating clinics are on the east coast of the U.S.; the association invites additional institutions to join.
The FDA already has a mechanism to ensure that risky drugs are safely administered. The Risk Evaluation and Mitigation Strategy (REMS) educates physicians on how best to use drugs with potential deleterious effects, and maintains a central database to track outcomes. Jason Karlawish of the University of Pennsylvania, Philadelphia, suggested the FDA require lecanemab use REMS. “The risk/benefit assessment is an ethically challenging Gordian knot. FDA and CMS should collaborate to assure this complicated drug’s transition from research into practice is net beneficial,” he wrote (full comment below).
In anticipation of approval and, potentially, insurance coverage, changes are already being set in motion across the research field. For example, leaders of longstanding observational cohorts that never disclosed amyloid status to their participants, such as AIBL and others, anticipate contacting them to inform them they can now find out their status and go on lecanemab if appropriate. Down's syndrome researchers are considering running trials in the readiness cohorts they have been building among this population. Scientists at drug companies across the field are starting to prepare for testing their investigational drugs against lecanemab as background medication. And aducanumab researchers are hinting that—just you wait—this antibody is going to come off the sidelines in 2023, as well.
All researchers Alzforum spoke with stressed that lecanemab and other amyloid immunotherapies represent the beginning of disease-modifying therapies. Many estimate a 30 percent slowing may be the most that can be achieved with amyloid removal alone in a symptomatic population, especially in the presence of mixed pathology. They emphasized the need to explore anti-amyloid drugs in presymptomatic populations with biomarker evidence of only amyloid pathology, or amyloid and tau pathology. All eventually want active vaccines to reduce cost and open treatment to large populations across nations. Finally, they urge combination trials of different therapeutic approaches to build on this first signal. At CTAD, Lefkos Middleton of Imperial College London said, “We need to celebrate what we have, but keep investigating AD biology to find treatments that make a big difference.”
Also at CTAD, Selkoe, Gil Rabinovici of the University of California, San Francisco, and several others, met to discuss how to rally support for lecanemab among policymakers in the U.S. and internationally. They drafted a joint letter that is being sent around within the community along with a sign-on form. The signature processes is being coordinated by Robert Egge at the Alzheimer's Association, which may use the letter to influence the U.S. Centers for Medicare and Medicaid Services. If the FDA approves lecanemab in 2023, the CMS will make a coverage decision that private insurers are likely to follow. —Madolyn Bowman Rogers & Gabrielle Strobel
References
News Citations
- ApoE4 and Tau in Alzheimer’s: Worse Than We Thought? Especially in Women
- Aducanumab Still Needs to Prove Itself, Researchers Say
- Aduhelm Phase 3 Data: ARIA Is Common, Sometimes Serious
- Lecanemab: FDA Set Accelerated Approval Decision for January 2023
- Aduhelm Lowers Tau; Registry to Track Real-World Performance
- Bringing Aduhelm—and Antibodies to Come—Into Practice
Therapeutics Citations
Paper Citations
- Winkler DT, Biedermann L, Tolnay M, Allegrini PR, Staufenbiel M, Wiessner C, Jucker M. Thrombolysis induces cerebral hemorrhage in a mouse model of cerebral amyloid angiopathy. Ann Neurol. 2002 Jun;51(6):790-3. PubMed.
- Pfeifer M, Boncristiano S, Bondolfi L, Stalder A, Deller T, Staufenbiel M, Mathews PM, Jucker M. Cerebral hemorrhage after passive anti-Abeta immunotherapy. Science. 2002 Nov 15;298(5597):1379. PubMed.
Other Citations
External Citations
Further Reading
News
- How Will Alzheimer’s Trials, Treatment Change in 2023 and Beyond?
- Bringing Aduhelm—and Antibodies to Come—Into Practice
- With Aduhelm in Retrenchment, Lecanemab Completes FDA Submission
- Using Lecanemab Trial Data to Determine Maintenance Dose
- Lecanemab Sweeps Up Toxic Aβ Protofibrils, Catches Eyes of Trialists
Primary Papers
- van Dyck CH, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, Kanekiyo M, Li D, Reyderman L, Cohen S, Froelich L, Katayama S, Sabbagh M, Vellas B, Watson D, Dhadda S, Irizarry M, Kramer LD, Iwatsubo T. Lecanemab in Early Alzheimer's Disease. N Engl J Med. 2023 Jan 5;388(1):9-21. Epub 2022 Nov 29 PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
Co-Director, Brigham and Women's Hospital's Ann Romney Center for Neurologic Diseases
Those who attended CTAD 2022 experienced the palpable excitement of the full presentation of the Phase 3 results on lecanemab. The findings need not be detailed here; fortunately , they underwent peer review contemporaneously and are in the NEJM. In my view, this is the outcome our field has long hoped for. The most impressive aspect of the study is the consistency of the results across the primary endpoint and four secondary endpoints: all showed significant (p<0.001) benefit over placebo.
The ADCS-MCI-ADL outcome may turn out to be particularly meaningful for our patients. The rising deltas of lecanemab vs. placebo over 18 months on all key endpoints suggest a reasonable likelihood of greater benefits at 24 months and beyond. Equally impressive were the consistent biomarker outcomes: substantial decreases in amyloid and NFT burdens by PET and benefits on their constituent proteins in CSF and plasma. I was particularly pleased to see the significant fall in plasma GFAP levels. This result suggests a notable amelioration of an inflammatory component (astrocytosis) that is increasingly recognized as a main feature of AD; a plasma biomarker of microgliosis may follow.
The sole clinically significant adverse effect was ARIA-E (ARIA-H did not independently contribute to the clinical impact of ARIA-E). The rate of symptomatic ARIA-E of 2.8 percent across ApoE genotypes suggests that experienced AD clinicians should be able to carefully mange this challenge with genotyping, MRI monitoring, and close communication with patients about what symptoms require an early call to the doctor.
The uniform trends toward less decline across clinical endpoints, coupled with substantial lessening of the lesions that define AD, indicate that disease modification has occurred, essentially proving the amyloid hypothesis as well as the disruptive concept of immunotherapy that Dale Schenk brought us.
I speculate that FDA review will lead first to accelerated approval (based on the Phase 2 results plus the safety dossier) followed by full approval of the Clarity AD data. I applaud Bioarctic for creating lecanemab and Eisai for completing very well-executed Phase 2 and 3 studies. There can be no doubt that we will continue to strive toward larger deltas over placebo and ultimately the arrest or prevention (e.g. through AHEAD) of symptoms.
But I believe the current clinical and biomarker outcomes provide clear-cut evidence of a useful disease-modifying agent. Its risk/benefit ratio represents a signal advance that we can build on, and which can be carefully discussed with the roughly 25 percent of AD patients who meet the Clarity AD entry criteria.
Mayo Clinic College of Medicine
The NEJM article and the oral presentation at CTAD on the results of the CLARITY trial with lecanemab 10 mg/kg Q2W were encouraging. The primary outcome, all of the secondary outcomes and the fluid and imaging biomarkers all were consistent with a modest benefit. In the appropriate patients, the medication may be of benefit.
The clinical meaningfulness of the delay in decline produced by lecanemab, just shy of about five months over the 18 months of the trial, may not be noticed by patients or families, but if the reduction in decline were to persist for, say, three to four years, I would expect it to be appreciated by families and patients. On the other hand, if the effect is not durable and fades within a year or so, there will be much less enthusiasm for its use, which after all is somewhat arduous. While we are waiting for the longer-term outcomes, I expect that its introduction into clinical practice will have a major impact on dementia care.
Washington University School of Medicine
I’m cautiously optimistic about the lecanemab data. Because there is such mild decline in these patients over 18 months, it’s very difficult to see a positive signal, particularly when it takes several months to titrate the medication and remove the plaque. Thus, I’m impressed the signal is so clear, even if it is small in an absolute sense. It remains to be seen if the placebo and treatment group curves will diverge further as the disease progresses. If so, the risk and cost/benefit of the drug could be very positive. If not, and 27 percent slowing is the best we are going to get, the economics and risk/benefit will be murkier.
I am encouraged that the Phase 2 trials for aducanumab, lecanemab, and donanemab, one of the Phase 3 trials for aducanumab, and now the Phase 3 trials for lecanemab, all show a similar positive signal and magnitude of effect. The failure of gantenerumab is disappointing, as the subcutaneous delivery would have been very advantageous, but suggests that there may be a threshold of plaque removal needed to see effect, which gantenerumab did not achieve.
The every-two-week treatment schedule of lecanemab is certainly a negative, as is the indefinite dosing duration, and hopefully these could be improved over time. We will see about cost. The two deaths are sobering and emphasize that this drug should probably not be mixed with anticoagulation or tPA usage, and is probably better suited for generally healthier patients. If I were to start using this in my clinic, I would target it at healthier patients with positive biomarkers but milder symptoms, less atrophy on MRI, no microhemorrhages, and no anticoagulation. Patients will need to be motivated, reliable, and have good access and support (as well as insurance) to successfully receive this therapy and keep up with the MRI monitoring.
Over time, we should develop protocols to select responsive patients more effectively, minimize risk, and improve access, but these systems will not be in place at first. However, we need to take a first step forward, and this could be it.
University of Pennsylvania
Lecanemab’s benefits are real. The drug shows consistent effects across measures of cognition, function, caregiver burden and even patient self-rated quality of life. This is impressive. So too are the changes in biomarkers of tau and Aβ.
Lecanemab’s risks of brain bleeding and swelling are real too. In fact, they’re really complicated, especially in persons who are APOE4 carriers. APOE4 carriers have a dose response decrement in benefit, the risk affects the very same organ the drug is treating, and an APOE result ramifies into a family.
As a clinician, I look forward to prescribing lecanamab for my patients at the Penn Memory Center. As a researcher in ethics and policy, I worry. The risk benefit assessment is an ethically challenging Gordian knot. FDA and CMMS should collaborate to assure this complicated drug’s transition from research into practice is net beneficial.
The crux of the problem is the lack a clinical infrastructure to deliver this drug. Memory centers such as where I practice are uncommon. Moreover, none of the measures of benefit are routinely used in clinical practice. Lecanemab is a hard drug to think through. Its measures of benefit are clinically opaque, dimensional measures of time-dependent experiences. Its risks are precisely measured, highly transparent events. This, together with the limited infrastructure of competent prescribers, could sink this promising drug.
The best way forward is to set up a system designed to mitigate the risks of unreasonable prescribing and detect hotspots of problematic use. FDA offers a mechanism to do this. Its Risk Evaluation and Mitigation System, or REMS, allows for the prescribing of medications with serious safety concerns to ensure the benefits of the medication outweigh its risks. FDA explains, “REMS focus on preventing, monitoring and/or managing a specific serious risk by informing, educating and/or reinforcing actions to reduce the frequency and/or severity of the event.” The lecanemab REMS would assure a clinician meets criteria of knowledge and skills, practices in a setting with the appropriate infrastructure to move the patient safely to infusion, and records risks in a centralized database.
One other ethical point needs to be addressed. Among the oddest interpretations of CLARITY is that FDA “got it right” with aducanumab. In other words, reduction of amyloid measured using PET is strong and sufficient evidence to grant a drug conditional approval for the treatment of persons living with Alzheimer’s disease.
It is presumptuous to claim the field has consensus that this measure of amyloid reduction is a surrogate akin to viral load, tumor size or blood pressure for the approval of treatments targeting HIV, cancer and heart disease, respectively.
At the CTAD panel on the Phase 3 trials of anti-amyloid drugs, Chris van Dyck, the lead author of the CLARITY paper in NEJM, offered a pithy summary why. He argued that clearance of amyloid as shown by PET scan may well not represent the mechanism of benefit. Instead, clearance of soluble amyloid may be the mechanism. Soluble amyloid is unmeasurable. Reduction of amyloid seen on PET is, he concluded, “a surrogate of a surrogate.”
Science offers us a reasonable way forward. The results of the lecanemab and gantenerumab studies have clues. It is quite possible that measures of tau, or of tau and amyloid together, may be the surrogates. Or maybe not. Listen to the data, not to assertions of power delivered from the podium.
Regulatory science can move this along. FDA should convene an advisory committee to consider the state of the evidence for amyloid clearance as a surrogate worthy of gatekeeping a drug for conditional approval. It should also consider whether we even need a surrogate.
There’s another disturbing problem with this claim that FDA “got it right.” It’s an assertion of revisionism that evokes the work of the Ministry of Truth.
Let us remember. FDA convened an advisory board to answer questions about regular—not conditional—approval. FDA officials publicly dismissed amyloid as a surrogate and held off-the-books meetings with Biogen employees, internal divisions at FDA were swept aside, there was no plan for a confirmatory trial, the initial label was so poorly constructed that it required revision.
We await the outcome of the Office of Inspector General’s investigation.
Dementia Reserch Center
This result will be seen as a historic moment in our field—the beginning of a new era to therapies for AD. It represents a more than 20-year effort and the work of many on this and on many other anti-amyloid immunotherapies.
The full data support the promise of disease modification that was press-released and indeed shown in the Phase 2b study back in 2018. The results confirm a robust effect of slowing of cognitive decline of 27 percent on the primary outcome. Not only did the trial hit is primary endpoint, but it also showed positive effects on a wide range of secondary outcomes, including benefit in terms of activities of daily living even in this very mild AD population.
As was to be expected, the treatment produced a dramatic reduction in brain amyloid as measured by PET. The level of amyloid PET binding hardly changed in the placebo arm but in the lecanemab arm binding fell to below the level of what is considered “positive,” in other words the reduction was so large that many or most participants would no longer have been eligible even to enter the study. On average they would no longer have had enough PET evidence of Alzheimer’s disease to fulfil inclusion criteria. This recapitulates the Phase 2b finding and what is seen in other therapies to lesser or greater extent, e.g., donanemab.
The study fits the idea that amyloid levels need to be reduced low enough, and for long enough, to see benefit on clinical measures. It is notable that the Phase 2b did not hit its primary outcome at 12 months but did so at 18 months. On just about every metric the Phase 2b predicted what was seen in this Phase 3 study, from the level of clinical benefit through to the proportion who would get ARIA-E.
A key question is whether clinical benefits continue, if they are sustained and cumulative, beyond 18 months. The trial was not powered to address whether benefits were progressive over the 18 months, but some graphs of change, e.g. on the primary outcome, do suggest a widening of the gap between treatment and placebo arms.
There have been lots of understandable concerns raised about safety of this class of therapies, in particular about the impact of ARIA-E seen on MRI. These do need to be taken seriously, but in a balanced way. ARIA-E refers to edema (swelling) and effusions seen on MRI that are likely a result of amyloid removal. Amyloid is widely distributed in the brain, including, importantly, in the walls of blood vessels in the brain.
The headline figure for ARIA-E in this trial is of 12.6 percent, i.e., 1 in 8, of those who received lecanemab, while 1.7 percent, fewer than 1 in 50, developed it in the placebo arm. I believe one needs to look beyond these numbers, at the number who had symptoms. Eighty percent of these ARIA-E cases had no discernible symptoms, and overall 2.8 percent, i.e. fewer than 1 in 30 had any symptoms (headaches, confusion etc). Notably, the number of deaths in the treatment and placebo arms were essentially identical, slightly fewer in those on lecanemab (0.7 percent) than on placebo (0.8 percent), and the study investigators did not feel that any of the deaths were related to treatment or ARIA.
Any risk is clearly important, but I believe many of my patients would be very willing to take such a risk, especially as most ARIA resolves within weeks. These treatments are, however, not for the faint-hearted. Intravenous infusions every two weeks is a real burden on families.
This is also a massive challenge to health systems, which will struggle with this therapy. Huge resources would be needed to deliver it, and many health systems do not currently have the investigation capacity to assess amyloid status by PET or CSF or even to provide the MRI scans needed for inclusion in the study and monitoring. In this trial, the participants had six MRI scans (weeks 9, 13, 27, 53, and 79 as well as at the three-month follow-up visit) for safety monitoring even for those without any ARIA.
If the benefits extend beyond 18 months, lecanemab does offer the potential of clinically meaningful benefits that could change the outlook for this devastating disease, but it raises lots of challenges:
- we will need to find ways of delivering therapies safely and more easily. Sub-cutaneous would be a step in the right direction.
- does treatment need to continue or can it be paused?
- how early should it be started?
- cumulative benefits logically mean that the earlier treatment is started, the greater the difference that is made in terms of preserving function for longer
- most of us would want our disease slowed when we still had a good quality of life and independent functioning; conversely, if disease slowing is delivered late we could prolong individuals in a dependent state
- we will need resources for timely assessment and investigation.
Until now we have only had symptomatic therapies for Alzheimer’s disease. That meant delays in starting treatment did not “cost brain cells" or alter ultimate outcomes. Unlike treatments for cancer, and many other areas of medicine, time was not of the essence. Now it is. I hope we can transform outcomes in Alzheimer’s disease as they have been with other hitherto “untreatable diseases.” The many challenges and problems to address, from cost to logistics to ethical questions, but for the millions of present and future patients globally, it’s better to have these problems than no problems and no prospects.
Disclosures: I have served on advisory boards/as consultant to Biogen, Eli Lilly, Ionis, Roche Siemens (all paid to UCL, not taken personally); Data Monitoring Safety Board for Biogen (for aducanumab); research support to our research center from Eli Lilly and Biogen; unpaid member of advisory boards for Alzheimer’s Research UK, Alzheimer’s Society.
University of Kansas
The extent to which the separation between the groups is an artifact of unblinding is difficult to say, but I think it is safe to conclude that over the 18 months the extent to which decline slowed was likely more than 0 percent and less than 30 percent. The percentage of people who experienced serious and sustained harm specifically from the drug itself is also hard to say but at face value the chances of the drug causing serious and sustained harm is not large but also not negligible. Based on what is reported here and also precedent, one would have to assume this drug will become available to the clinic in 2023.
Others will disagree, but I would not conclude this study addresses the cause or causes of Alzheimer’s disease. I would say this study does imply that Aβ, perhaps in the form of plaques, can itself have a limited adverse effect on cognitive function. Whether the clinical benefit now reported reflects true disease modification, or the indirect modification of another biology such as inflammation, is also arguably unsettled. Over the coming years it will be interesting to see how many AD patients and their families conclude their lives were favorably transformed by this drug versus unfavorably transformed by this drug.
Regarding the upside/downside analysis, the reported efficacy signal is coincidentally in the range of what has previously been reported for a vitamin E intervention trial (Dysten et al, 2014). Vitamin E is relatively safe, it is inexpensive, and it generated little interest. The fact that lecanemab is making such a stir relative to vitamin E may reflect the ongoing conflation of amyloid with AD. Given data emerging from donanemab and ganteranumab trials, many will no doubt argue it is clear to beat AD we need to aggressively remove plaques from the brain. However, where does the field go if patients cleared of plaques continue to decline? In other words, since the most promising antibodies seem to robustly remove plaques, does this imply the benefit ceiling of the monoclonal antibody approach is likely quite low?
References:
Dysken MW, Sano M, Asthana S, Vertrees JE, Pallaki M, Llorente M, Love S, Schellenberg GD, McCarten JR, Malphurs J, Prieto S, Chen P, Loreck DJ, Trapp G, Bakshi RS, Mintzer JE, Heidebrink JL, Vidal-Cardona A, Arroyo LM, Cruz AR, Zachariah S, Kowall NW, Chopra MP, Craft S, Thielke S, Turvey CL, Woodman C, Monnell KA, Gordon K, Tomaska J, Segal Y, Peduzzi PN, Guarino PD. Effect of vitamin E and memantine on functional decline in Alzheimer disease: the TEAM-AD VA cooperative randomized trial. JAMA. 2014 Jan 1;311(1):33-44. PubMed.
USC Alzheimer’s Therapeutic Research Institute
I was pleased that the presentation on lecanemab at CTAD was received with almost uniform excitement and enthusiasm. With intervention at the early AD stage, we can slow AD progression by 27 percent, a clearly meaningful benefit. Functional decline slows by 36 percent. The biomarker results demonstrate beneficial effects on the neurobiology of AD. The potential for ARIA requires monitoring but overall risks are manageable.
The gantenerumab results, together with the Prime, Emerge, Engage, Trailblazer and the Phase 2 lecanemab results tell a consistent story. Normalizing fibrillar amyloid as measured by PET, with mean SUVr after treatment below 30 centiloids, is associated with slowing of clinical progression. If amyloid reduction is less robust clinical benefits may not be seen.
The Clarity AD trial is a landmark in AD therapeutic research, the culmination of over three decades of efforts across the field. Now we must build on this success by studying add-on therapies and earlier intervention.
Acumen Pharmaceuticals
The presentation of the Clarity AD trial results at CTAD this year represents a seminal change in the field of AD research. The positive results for clinical outcomes in the study are most important, but the history and development of the program are equally important points of learning for AD researchers.
Lecanemab, previously known as BAN2401, was developed as an antibody generated against a unique antigen, Ab protofibrils (Lannfelt et al., 2014) The basis of this antigen was recognized by Dr. Lars Lannfelt, given the effects seen from the “Arctic mutation” in APP that he identified in Sweden. Patients with this mutation developed AD dementia, but had diffuse rather than neuritic plaques, and additional studies subsequently showed that the protofibrils generated by the Arctic mutation were soluble and toxic to neurons. The first Phase 1/2a study using BAN2401 was initiated in 2010 with 80 patients (60 active:20 placebo) with doses up to 15 mg/kg. Following this study, a Phase 2 study using a complex adaptive design with a Bayesian analysis was initiated in 2013. While the primary analysis for this study was negative, secondary analyses using more traditional statistical techniques were positive, and the decision was made to proceed to the Phase 3 Clarity AD trial, which started in 2019.
Given the history of BAN2401, now known as lecanemab, attention to an antibody targeting protofibrils has previously been relatively limited. The appreciation of this target has increased substantially given the Clarity AD results presented at CTAD. As reported widely, in this study of patients with mild cognitive impairment (MCI) or mild AD dementia due to AD, intravenous lecanemab given every two weeks over 18 months led to statistically significant (p<0.001) slowing of cognitive and functional decline based on the CDR-SB, which was the primary outcome. Additionally, three secondary outcomes, the ADAS-cog14, ADCOMS, and the ADCS-MCI-ADL scores reached nominal statistical significance. Importantly, various sensitivity analyses showed similar effects, supporting the primary and secondary study results. While some subgroups may show more or less efficacy as shown in Forest plots presented at CTAD, little if any debate is necessary regarding the overall efficacy of the drug.
While a debate on the overall efficacy based on the CDR-SB primary and secondary outcomes is not necessary, a discussion of the clinical meaningfulness of this effect has already begun. The difference between active treatment and placebo in Clarity AD is 0.45 points on the CDR-SB after 18 months of treatment. The challenge that has been raised with regard to the clinical meaningfulness of this difference is that the CDR-SB is an 18-point scale in total and that a 0.45 change versus a total scale of 18 points might not be clinically important. This comparison is not relevant, however, as illustrated by the fact that the Fahrenheit scale is nominally 212 degrees, but a 3-degree change in temperature in a human is clearly clinically meaningful. Based on recent studies of early AD patients similar to those included in Clarity AD, the expected rate of decline in the CDR-SB in one year is slightly more than 1.0 (Budd Haeberlein et al., 2022; Mintun et al., 2021)
Thus, a difference of 0.45 points represents a difference of almost six months of decline for patients with early AD. The vast majority of clinicians seeing patients with early AD, as well as their patients and families, are likely to endorse the idea that six months of decline is clinically meaningful.
Regarding safety, ARIA-E occurred in 12.6 percent of lecanemab recipients and 1.7 percent of those on placebo overall. Interestingly, the ARIA-E rate was lower than in previous trials of antibodies that target amyloid plaques (e.g. aducanumab and donanemab) directly. This suggests that the different targets for lecanemab (protofibrils) and aducanumab and donanemab (amyloid plaques) result in important differences is safety profiles.
The results of Clarity AD will be provided for a full priority review for FDA and we hope will engender a rapid review by other regulatory agencies. Further, the clinical meaningfulness of the results will hopefully include a rapid review for reimbursement by the Center for Medicare and Medicaid Services (CMS) and other payors outside the U.S. A major conclusion from this study is that Clarity AD has provided a major inflection point for the field, and we need to build on this success to provide even greater benefits to AD patients and their families.
References:
Lannfelt L, Relkin NR, Siemers ER. Amyloid-ß-directed immunotherapy for Alzheimer's disease. J Intern Med. 2014 Mar;275(3):284-95. PubMed.
Budd Haeberlein S, Aisen PS, Barkhof F, Chalkias S, Chen T, Cohen S, Dent G, Hansson O, Harrison K, von Hehn C, Iwatsubo T, Mallinckrodt C, Mummery CJ, Muralidharan KK, Nestorov I, Nisenbaum L, Rajagovindan R, Skordos L, Tian Y, van Dyck CH, Vellas B, Wu S, Zhu Y, Sandrock A. Two Randomized Phase 3 Studies of Aducanumab in Early Alzheimer's Disease. J Prev Alzheimers Dis. 2022;9(2):197-210. PubMed.
Mintun MA, Lo AC, Duggan Evans C, Wessels AM, Ardayfio PA, Andersen SW, Shcherbinin S, Sparks J, Sims JR, Brys M, Apostolova LG, Salloway SP, Skovronsky DM. Donanemab in Early Alzheimer's Disease. N Engl J Med. 2021 May 6;384(18):1691-1704. Epub 2021 Mar 13 PubMed.
UC Irvine Institute for Memory Impairments and Neurological Disorders
I think the results presented at CTAD were convincing and noteworthy on several levels:
1) The primary and key secondary outcomes were consistent. I was impressed by the reduced decline on the ADCS-ADL-MCI, indicating that patients and families could benefit from slowing of observable functional worsening.
2) The sensitivity analyses addressed important issues related to potential unblinding due to ARIA (even if asymptomatic) and COVID.
3) The subgroup analyses were largely consistent in suggesting benefit in most subgroups. There are questions about lack of significance in some of the subgroups, but what stood out to me was that APOE e4 homozygotes did not seem to benefit. Combined with much higher ARIA rates in this subgroup (see below), there will be important conversations about why this group may not have benefited in this trial and how appropriate it will be to use lecanemab in them, if it is approved. Maybe more important will be understanding why some subgroups may not have benefited. Was in inadequate lowering of amyloid? Was it too high of amyloid burden at baseline? Or was it some other downstream marker of benefit?
4) The biomarker results were exciting for the observed benefits on some outcomes (e.g., CSF tau and GFAP) and intriguing for the lack of effects in others (e.g., CSF NfL).
5) The time-to-event model presented in the symposium (Figure S6 in the NEJM publication) seems particularly important. It appears that the groups may be increasing in difference over time (though the n’s are greatly reduced and no confidence intervals are provided). But it also appears that the lecanemab group may “catch up” with placebo after three to six months. Understanding the clinical meaningfulness of treatment and how to describe it to patients and families will be particularly important moving forward.
6) I view the safety profile to be acceptable. The double-bind portion of the study is most important to this assessment at this time. ARIA remains the main adverse event of interest and it was higher in the lecanemab arm of the study and higher in APOE e4 carriers. People will need to be informed of their risk when taking lecanemab if it is approved and this will likely mean APOE genotyping and a more complicated practice that ideally involves genetic counselors and then monitoring for ARIA.
7) Finally, the data were presented with rigor and balance and a peer-reviewed publication was released simultaneously. This replicates some previous Phase 3 result presentations and avoids the missteps of other predecessors.
Combined with the Gantenerumab Phase 3 data, the head-to-head results of donanemab vs. aducanumab presented, and several other outstanding presentations made at the meeting, it is clear that the field is entering a new and extremely exciting phase of treatment development. The data do not, in my opinion, prove that amyloid PET can or should be used as a surrogate outcome. Instead, as we move toward better therapies and possible combinations of therapies, clinical outcomes will remain supreme, though downstream markers of tangle burden or neurodegeneration may become even more important when amyloid therapies are in use and capable of bringing someone down to “not elevated” levels (below 20-25 centiloids).
So far, disease-modifying therapies are not disease-stopping therapies. Helping patients and families understand this, and the urgent need for them to participate in trials moving forward, will remain of the utmost importance.
Sorbonne University - APHP - Pitié-Salpêtrière Hospital
The lecanemab’s Phase 3 results are the highest-quality and consistent dataset that has been disclosed and published so far on anti-amyloid immunotherapies in early AD. The results and methodology are univocal and cannot be disputed. Eisai revealed additional details in the CTAD presentation that reinforced the core statistics and message from the NEJM article. We can only be satisfied after the aducanumab disaster!
As a scientist, I can only be delighted by these unambiguous results representing a breakthrough in AD therapeutics: the use of mAbs directed against a peptide expected to play a role in AD pathogenesis did slow down disease progression!
As a physician, I have mixed feelings about this drug’s risk/benefit ratio. Regarding benefits, after 18 months, we observe a 0.45 difference in CDR-SB between the two groups, which is far below the minimal clinically important differences (MCID) that have been previously established by the industry and have consistently set this difference to 1 point in this population (Andrews et al., 2019; Lansdall et al., 2022). Effects on quality of life are, of course, encouraging, but recent literature reviews regarding those scales challenge their relevance in AD clinical trials (El-Hayek et al., 2019).
If this drug is an actual disease-modifying therapy (DMT), this 0.45 difference will progressively increase with time to reach MCID. Contrary to Randy Bateman, I would not be as assertive as to claim that there is enough evidence for disease modification. As underlined in the text above, the slope analysis after 12 months is not in favor of DMT, while not all biomarkers regarding neurodegeneration show consistent findings. Finally, no correlation or mediation analysis demonstrates the relationship between these biomarkers and cognitive performance. Postmortem observations of brains with high clearance of Aβ and late stages of tauopathy and neurodegeneration from the anti-amyloid vaccine AN1792 trials might support these doubts about lecanemab’s disease modification (Boche et al., 2010; Nicoll et al., 2019). If the absolute 0.45 points, and not the relative 27 percent, difference in CDR-SB were the actual maximum difference that could be reached with lecanemab, it would limit its clinical relevance.
Regarding safety, as underlined in the text above, three severe ARIA cases have been reported during the CTAD presentation. Besides, 10/898 (1.1 percent) individuals were classified as having serious adverse events with ARIA (Michael Irizarry, personal communication). Two of these cases occurred in our center, and we described them in a paper published last September (Fig 3. from Villain et al., 2022). I saw the patient with the serious ARIA-H two weeks ago: her MMSE is now 4/30, 18 months after the ARIA. These severe ARIA have long-term sequelae and represent a substantial loss for the patient.
The actual rate of these severe ARIA remains unknown. But this occurred despite the strict exclusion criteria and the close in-trial monitoring. In real-life clinical practice, this rate might increase. Like Jason Karlawish, I advocate for a REMS to monitor these events and gather enough data to define the subgroups/algorithm that will help to estimate these risks in the future better.
Overall, this drug’s risk/benefit ratio can be questioned. Especially for regulators and payors, considering the high prevalence of AD and the provisional total high costs and complexity of lecanemab’s implementation in any healthcare system.
Finally, the history of medicine reminds us that first-in-class drugs can have unfavorable risk/benefit ratios (e.g., AZT as a single therapy for HIV, tacrine for AD …) but are the trigger for the subsequent development of new drugs or combination therapies with better risk/benefit ratios. The Eisai CEO's recent intervention makes me optimistic. He demonstrates the sponsor’s willingness to consider these concerns when claiming that “this is not a cure” and advocating for a careful prescription in APOE4 homozygous. Identifying—and possibly, as a first step, limiting—indications to subgroups with better risk/benefit ratios, and better demonstration of disease modification in new delayed-start clinical trials, may be solutions to better align patients, sponsor, prescribers, regulator, and payor’s concerns.
This can be a huge step for the field and the patients: Let’s make it right!
References:
Andrews JS, Desai U, Kirson NY, Zichlin ML, Ball DE, Matthews BR. Disease severity and minimal clinically important differences in clinical outcome assessments for Alzheimer's disease clinical trials. Alzheimers Dement (N Y). 2019;5:354-363. Epub 2019 Aug 2 PubMed.
Boche D, Denham N, Holmes C, Nicoll JA. Neuropathology after active Abeta42 immunotherapy: implications for Alzheimer's disease pathogenesis. Acta Neuropathol. 2010 Sep;120(3):369-84. PubMed.
El-Hayek YH, Wiley RE, Khoury CP, Daya RP, Ballard C, Evans AR, Karran M, Molinuevo JL, Norton M, Atri A. Tip of the Iceberg: Assessing the Global Socioeconomic Costs of Alzheimer's Disease and Related Dementias and Strategic Implications for Stakeholders. J Alzheimers Dis. 2019;70(2):323-341. PubMed.
Lansdall CJ, McDougall F, Butler LM, Delmar P, Pross N, Qin S, McLeod L, Zhou X, Kerchner GA, Doody RS. Establishing Clinically Meaningful Change on Outcome Assessments Frequently Used in Trials of Mild Cognitive Impairment Due to Alzheimer’s Disease. The Journal of Prevention of Alzheimer's Disease, December 8, 2022 The Journal of Prevention of Alzheimer's Disease
Nicoll JA, Buckland GR, Harrison CH, Page A, Harris S, Love S, Neal JW, Holmes C, Boche D. Persistent neuropathological effects 14 years following amyloid-β immunization in Alzheimer's disease. Brain. 2019 Jul 1;142(7):2113-2126. PubMed.
Villain N, Planche V, Levy R. High-clearance anti-amyloid immunotherapies in Alzheimer's disease. Part 1: Meta-analysis and review of efficacy and safety data, and medico-economical aspects. Rev Neurol (Paris). 2022 Dec;178(10):1011-1030. Epub 2022 Sep 29 PubMed.
University of Cincinnati
One crucial variable remains invisible in the discussion of this important trial: CSF Aβ42 levels. Lecanemab significantly increased these levels in Phase 2 and Phase 3 trials (Supplementary Figure 5 in the NEJM publication). Understanding the changes in clinical endpoints warrants measuring both ends of the protein state: the soluble Aβ42 in pg/ml in CSF (the more functional and fibrillogenic of the Aβ species), which begins to deplete decades before symptom onset, and the insoluble amyloid in PET-measured centiloids. Analyzing only one of these tells half the story.
While the relationship between amyloid positivity and dementia only reaches a 5:1 ratio by age 85 (Jack et al., 2019) that of low soluble Aβ42 is 1:1. This means that most of us with amyloid can walk around without neurological symptoms throughout our life but not a single one of us with dementia will have high Aβ42.
Might Eisai/Biogen be willing to analyze the extent to which the clinical changes may be mediated more by changes in soluble Aβ42 than by changes in amyloid centiloids? We hypothesize that lecanemab responders may disproportionally be among those with increases in soluble Aβ42 above a certain threshold of compensation, i.e. >800 pg/ml in amyloid-positive ADNI participants (Sturchio et al., 2021) and >270 pg/ml in amyloid-positive DIAN participants (Sturchio et al., 2022).
References:
Jack CR Jr, Therneau TM, Weigand SD, Wiste HJ, Knopman DS, Vemuri P, Lowe VJ, Mielke MM, Roberts RO, Machulda MM, Graff-Radford J, Jones DT, Schwarz CG, Gunter JL, Senjem ML, Rocca WA, Petersen RC. Prevalence of Biologically vs Clinically Defined Alzheimer Spectrum Entities Using the National Institute on Aging-Alzheimer's Association Research Framework. JAMA Neurol. 2019 Jul 15; PubMed.
Sturchio A, Dwivedi AK, Young CB, Malm T, Marsili L, Sharma JS, Mahajan A, Hill EJ, Andaloussi SE, Poston KL, Manfredsson FP, Schneider LS, Ezzat K, Espay AJ. High cerebrospinal amyloid-β 42 is associated with normal cognition in individuals with brain amyloidosis. EClinicalMedicine. 2021 Aug;38:100988. Epub 2021 Jun 28 PubMed.
Sturchio A, Dwivedi AK, Malm T, Wood MJ, Cilia R, Sharma JS, Hill EJ, Schneider LS, Graff-Radford NR, Mori H, Nübling G, El Andaloussi S, Svenningsson P, Ezzat K, Espay AJ, Dominantly Inherited Alzheimer Consortia (DIAN). High Soluble Amyloid-β42 Predicts Normal Cognition in Amyloid-Positive Individuals with Alzheimer's Disease-Causing Mutations. J Alzheimers Dis. 2022;90(1):333-348. PubMed.
TrueBinding
We have made remarkable progress in terms of plasma and imaging biomarkers, as shown by treatment with lecanemab. This antibody was raised against Aβ protofibrils, which is a mixture of high molecular weight oligomers and fibrils (50-250KD). I am wondering about the effect of lecanemab on low molecular weight oligomers, particularly diners, trimers, and tetramers, which have greater toxicity profile than protofibrils.
The ARIA-E rate of 12.6 percent of lecanemab recipients is still high. In considering safety, we should focus not only on cognitive function and amyloid plaque load but also on auto inflammatory side effects.
The crucial question seems to me: Do these data already provide the maximal possible clinical efficacy of an Aβ pathology targeting antibody? In order to approach an answer to this question, it could be helpful to discuss the mode of action first. The time the course of lecanemab Phase 3 data may disclose some inherent information. The relative efficacy (Figure in NEJM paper) at the individual time points beginning with the statistically different six-months value calculates between 25 percent and 30 percent and is maintained across all four later time points of the study. There is no trend for an increase or decrease.
Obviously neither the decreasing amyloid plaque burden, nor the changing environment via dissolved Aβ species during the trial period, have an impact on the efficacy range of the antibody. These data are within expectations of a Dysfunction Hypothesis (Hillen 2019), but less explainable by the classical Amyloid Cascade Hypothesis (Hardy and Higgins, 1992) that renders Aβ deposit burden a central role in the course of the disease.
The Amyloid Dysfunction Hypothesis asks for more than an antibody that dissolves amyloid burden. Expecting full neutralization of pathology from the very beginning of treatment, the optimal Aβ antibody for AD prevention needs to be highly potent, and strictly isoform-selective for early Aβ misfolded conformations only. It should be optimized for CNS availability and early and maximal Tau biomarker response in a clinical POC study.
So far, I cannot see why 27 percent efficacy in this study should be a maximal effect for an Aβ-targeted therapeutic reagent. This is a good outlook for all patients and scientists, provided we learn from the failures of the past two decades and are willing to better understand the molecular mechanisms of meaningful Aβ physiology and pathology in AD.
Along this way, recent papers about the essential role of nascent Aβ monomer in human neurons with AD-linked APP-Swedish mutations (Zhou et al., 2022), as well as rescue functions of plaques (Huang et al., 2021), were encouraging. Hopefully these papers will trigger a new chapter in best practice therapy of meaningful Aβ pathology in AD.
References:
Hardy JA, Higgins GA. Alzheimer's disease: the amyloid cascade hypothesis. Science. 1992 Apr 10;256(5054):184-5. PubMed.
Hillen H. The Beta Amyloid Dysfunction (BAD) Hypothesis for Alzheimer's Disease. Front Neurosci. 2019;13:1154. Epub 2019 Nov 7 PubMed.
Huang Y, Happonen KE, Burrola PG, O'Connor C, Hah N, Huang L, Nimmerjahn A, Lemke G. Microglia use TAM receptors to detect and engulf amyloid β plaques. Nat Immunol. 2021 May;22(5):586-594. Epub 2021 Apr 15 PubMed.
Zhou B, Lu JG, Siddu A, Wernig M, Südhof TC. Synaptogenic effect of APP-Swedish mutation in familial Alzheimer's disease. Sci Transl Med. 2022 Oct 19;14(667):eabn9380. PubMed.
UC, Irvine
As noted in Alzforum's weekly newsletter today, lecanemab does increase the risks of brain swelling and bleeding, particularly in patients with APOE4 genotype. It should be noted that the National Institute of Neurological Disorders and Stroke (NINDS) and National Institute on Aging (NIA) are very interested in improving the safety of anti-Aβ monoclonal antibody treatments. Toward that goal of reducing the safety risks/adverse events associated with anti-Aβ immunotherapeutic approaches, NINDS and NIA recently released a Funding Opportunity Announcement (FOA) PAR-22-235: Blood Brain Barrier Response to Antibodies Targeting Beta-Amyloid (R01).
This FOA solicits applications designed to increase understanding of cellular and molecular mechanisms that can be targeted to protect the blood-brain barrier, and thus brain blood vessels, during therapeutic interventions that target Aβ. This includes applications that promote the discovery of cellular and molecular mechanisms that underlie brain blood vessels' responses to passive anti-Aβ immunotherapy that results in ARIA-E and H and other potentially adverse cerebrovascular responses. Up to three large R01 grants will be funded for five years to identify the causes of the anti-Aβ adverse events, and to develop effective supplemental treatments to improve the safety of anti-Aβ monoclonal antibody treatments, such as lecanemab.
IUPUI
The success of any therapy for Alzheimer's was way overdue. It has been 20 long years without a single successful new drug. Lecanemab's data were quite compelling. All primary and secondary outcomes were met and all biomarkers moved in the expected direction. This is truly our very first step towards curing Alzheimer's one day.
Amidst the excitement though, we should also note that we as physicians must prescribe this drug responsibly and counsel patients carefully about the risks and benefits. It is our responsibility to make sure lecanemab is safely administered and any ARIA and other side effects are promptly addressed. Getting a new drug on the market is half the battle of the launch. Using it responsibly is the next big task and we as neurologists will have to step up and not let our patients down.
Make a Comment
To make a comment you must login or register.